Internal injuries often are not immediately diagnosed. Injuries caused by motor vehicle accidents, blunt traumas, falls, penetrating wounds, bicycle accidents and even amusement park rides can all cause injuries to the liver, stomach, colon, spleen, pancreas and other internal organs. Often, internal bleeding happens slowly and can be very hard to diagnose. It often follows an accident, but can show up days after.
When You've Been Injured In An Auto Accident...
Unfortunately, the odds of you or a loved one being in a car accident during your lifetime are high. The impact an accident can have your life and your health can be devastating. Lost wages, chronic injuries (including broken bones, facial fractures, head trauma, traumatic brain injuries and paralysis), loss of a loved one and the financial toll of a collision can make the life you enjoyed before drastically different from the life you face after. When an accident is caused by a drunk driver or a driver under the influence of drugs or alcohol, the emotional toll can be overwhelming. Crashes often are caused by repeat DUI (drive under the influence) and DWI (drive while intoxicated) offenders, which makes it even harder to accept.
Internal injuries, especially those involving the liver, spleen, stomach, colon, pancreas and blood vessels can be caused by motor vehicle accidents, blunt trauma or penetrating injuries. For, example, the blunt, shearing force of striking the steer wheel in a motor vehicle accident lead to a significant amount of traumatic internal injuries. Other causes for traumatic internal, abdominal injury includes falls, striking injuries to the abdomen and penetrating wounds such as gunshots and stabbings.
The functions of the liver, blood storage and filtration, secretion of bile, breakdown of fats and regulation of blood volumes and clotting factors can all effected with injury to the liver. An accident victim with an injury to the liver may experience pain in the right upper abdominal region or upper abdomen area. Because the liver receives approximately one fifth of the blood pumped out of the heart, any bleeding injury to the liver can cause a significant blood loss from the liver. If this were to happen, the person’s blood pressure might fall, their abdomen may distend as it is filling with blood. The persons pulse can become weak and thready. Occasionally, if the liver injury is very small, the person may be admitted to the hospital for observation only. A major liver injury, may require immediate surgical intervention.
Blunt trauma to the abdomen can also result in injury to the spleen. The functions of the spleen, storing blood, freeing blood from wastes and organisms and storing hemoglobin, may all be distributed with an injury to the spleen. Because the spleen stores and maintains storage of blood, large amounts of blood can spill into the abdominal cavity after an injury to the spleen. A large volume of blood may be lost and the situation can become life threatening. Accident victims with an injury to the spleen may complain of left upper abdominal pain. Occasionally, this pain will radiate to the left shoulder. Due to blood loss, a person may also exhibit low blood pressures, weak pulse and possible bruising to the left upper abdominal area.
Injuries to the stomach are frequently caused by penetrating wounds or blunt force trauma. Frequently, injuries to the stomach occur with additional injuries to the pancreas or intestines. If there is injury to the stomach, the enzymes and acids that are secreted to assist with digestion leak into the abdominal cavity. This leakage of fluid can result in an infection. Injury to the stomach also interferes with the digestion of food. People with an injury to their stomach may complain of pain in the upper, mid abdominal area. Stomach injuries may also cause the person to have muscle guarding of the abdominal area, tenderness to touch, fast pulse and a low blood pressure.
Injuries to the pancreas often occur in conjunction with other abdominal injuries. Injury to the pancreas can have a high mortality rate that may be associated with a late diagnosis of the problem. Injuries to the pancreas alter its ability to perform its main functions of enzyme and insulin secretion. Accident victims with pancreatic trauma can complain of pain in the mid abdominal area or back. Abdominal guarding and low blood pressures may be present. Accident victims may have delayed symptoms of up to 12 hours after the initial injury, and making diagnosis difficult.
Injuries to the colon and bowels are most frequently because of blunt trauma, such striking the steering wheel in a motor vehicle accident. However, penetrating trauma also accounts for some injury to the colon. Injury to the colon disrupts the ability for the colon to assist with food breakdown, nutrient absorption and waste excretion. It is also possible for wastes and enzymes to leak from a damaged colon resulting in an infection of the abdominal area. Accident victims with injury to the colon may experience pain in the abdomen, nausea, vomiting, muscle guarding or tenderness, absence of bowel sounds or shock.
Blunt trauma is a major cause for damage to the large blood vessels internally. This includes motor vehicle accidents and falls. The acceleration/deceleration injury involved causes a shearing action and results in tears of the large blood vessels. Injury to these vessels (aorta, femoral and iliac vessels) results in a very large amount of blood loss. Accident victims with injury to the large vessels may complain of abdominal pain, nausea, and vomiting. On examination, an accident victims may have an increase in the size of their abdomen as it is filling with blood, abdominal tenderness, bruising in the abdomen, and/or falling blood pressure with shock. Accident victims may require immediate surgical intervention.
Accident victims with internal injury are at greater risk for bleeding and death. Sometimes these injuries may go undetected due to their vague symptoms and the fact that one can not visualize the injuries as they could a cut to the skin.
Tuesday 28 June 2011
Tuesday 21 June 2011
Internal Injuries
Internal Injuries
When people think of a typical a car accident, they usually don’t think of internal injuries. Unfortunately, the potential for some form of internal organ damage does exist and the results could be very serious. In fact, if left untreated, they can even be fatal. Following a serious motor vehicle accident, any number of internal organs can be impacted in various ways. Some of the more common internal organs that can be affected include the lungs, liver, bladder, kidneys, spleen and brain. The resulting internal injuries could take the form of such things as brain damage, a torn spleen, fractured ribs or even punctured lungs.
Internal Organs
Internal injuries from a car accident include injuries to bowels, kidneys, the spleen, liver, lungs, heart or aorta. Fractured ribs are quite common and may also puncture lungs and other internal organs. Torn spleens are also a frequent injury and may require extensive hospitalization.
Upper limbs
Hands, forearms, arms, shoulders, wrists and fingers are often injured in car accidents as well. Fractures are typical and treatment generally involves splints and casts. Occasionally, such injuries will require surgery in addition to splinting and casting. Therapy may also be required for increasing reduced strength and range of motion.
Rotator cuff injuries are frequently caused by car accidents. MRI scans are often used to diagnosis rotator cuff tears but since these tests are costly doctors will typically not order them immediately after a car accident and will wait for completion of physical therapy before ordering an MRI. Severe shoulder injuries will require shoulder reconstruction.
Lower limbs
Hips, legs, knees, heels, ankles, and feet are also commonly damaged in car accidents. Achilles tendon injuries, ankle sprains, collateral ligament injuries and stress fractures are typical. Fractures of the pelvis, femur, patella, tibia, and ankle may require casting or surgery. For serious hip and knee injuries, total hip replacements or total knee arthroplasty may be necessary after a car accident.

Soft Tissue Injuries
Injuries involving the internal organs are often caused by the impact of an auto accident, or by a broken rib that punctures an organ. Injuries can occur to the kidneys, liver, spleen, intestines, lungs, or heart, and may require extensive corrective surgery. In severe cases, certain internal injuries may lead to lifelong disability. Other injuries to the skin, such as cuts, scrapes, and abrasions, may require plastic surgery to correct.
Spinal Cord Injury
Auto accidents are one of the leading causes of spinal cord injury (SCI). The effects of spinal cord injuries vary based on the location and severity of the damage. In auto accidents, SCI is most often caused by excessive pressure, bruising, and lacerations involving the spinal cord. When severe, spinal cord injuries can radically change the life of the victim, causing some degree of paralysis or loss of muscle function in various areas of the body.
Victims of spinal cord injury face extensive challenges to restore their quality of life, and may require long term physical and occupational therapy, attendant care, pain medications, prosthetics, and more. Additionally, more than 30 percent of spinal cord injury patients require hospital admission every year for surgery, infections, respiratory complications, and other medical issues.
Traumatic Brain Injury
Car accidents are also one of the main causes of traumatic brain injury (TBI). During auto accidents, TBIs are caused either by a concussion when the victim’s head hits the inside of the vehicle, or from a serious whiplash injury that damages the brain tissues. Short and long term symptoms can include an altered state or loss of consciousness, memory loss, headaches, dizziness, vomiting, blurred vision, loss of smell, hearing, or taste sensations, speech problems, fatigue, depression, anxiety, and an increased sensitivity to light, noise, or movement. Even with years of rehabilitation and therapy, a person suffering from a traumatic brain injury may still require daily attendant care and life long medical treatments. The financial costs can be overwhelming for both the victims and their families.
When people think of a typical a car accident, they usually don’t think of internal injuries. Unfortunately, the potential for some form of internal organ damage does exist and the results could be very serious. In fact, if left untreated, they can even be fatal. Following a serious motor vehicle accident, any number of internal organs can be impacted in various ways. Some of the more common internal organs that can be affected include the lungs, liver, bladder, kidneys, spleen and brain. The resulting internal injuries could take the form of such things as brain damage, a torn spleen, fractured ribs or even punctured lungs.
Internal Organs
Internal injuries from a car accident include injuries to bowels, kidneys, the spleen, liver, lungs, heart or aorta. Fractured ribs are quite common and may also puncture lungs and other internal organs. Torn spleens are also a frequent injury and may require extensive hospitalization.
Upper limbs
Hands, forearms, arms, shoulders, wrists and fingers are often injured in car accidents as well. Fractures are typical and treatment generally involves splints and casts. Occasionally, such injuries will require surgery in addition to splinting and casting. Therapy may also be required for increasing reduced strength and range of motion.
Rotator cuff injuries are frequently caused by car accidents. MRI scans are often used to diagnosis rotator cuff tears but since these tests are costly doctors will typically not order them immediately after a car accident and will wait for completion of physical therapy before ordering an MRI. Severe shoulder injuries will require shoulder reconstruction.
Lower limbs
Hips, legs, knees, heels, ankles, and feet are also commonly damaged in car accidents. Achilles tendon injuries, ankle sprains, collateral ligament injuries and stress fractures are typical. Fractures of the pelvis, femur, patella, tibia, and ankle may require casting or surgery. For serious hip and knee injuries, total hip replacements or total knee arthroplasty may be necessary after a car accident.

Soft Tissue Injuries
Injuries involving the internal organs are often caused by the impact of an auto accident, or by a broken rib that punctures an organ. Injuries can occur to the kidneys, liver, spleen, intestines, lungs, or heart, and may require extensive corrective surgery. In severe cases, certain internal injuries may lead to lifelong disability. Other injuries to the skin, such as cuts, scrapes, and abrasions, may require plastic surgery to correct.
Spinal Cord Injury
Auto accidents are one of the leading causes of spinal cord injury (SCI). The effects of spinal cord injuries vary based on the location and severity of the damage. In auto accidents, SCI is most often caused by excessive pressure, bruising, and lacerations involving the spinal cord. When severe, spinal cord injuries can radically change the life of the victim, causing some degree of paralysis or loss of muscle function in various areas of the body.
Victims of spinal cord injury face extensive challenges to restore their quality of life, and may require long term physical and occupational therapy, attendant care, pain medications, prosthetics, and more. Additionally, more than 30 percent of spinal cord injury patients require hospital admission every year for surgery, infections, respiratory complications, and other medical issues.
Traumatic Brain Injury
Car accidents are also one of the main causes of traumatic brain injury (TBI). During auto accidents, TBIs are caused either by a concussion when the victim’s head hits the inside of the vehicle, or from a serious whiplash injury that damages the brain tissues. Short and long term symptoms can include an altered state or loss of consciousness, memory loss, headaches, dizziness, vomiting, blurred vision, loss of smell, hearing, or taste sensations, speech problems, fatigue, depression, anxiety, and an increased sensitivity to light, noise, or movement. Even with years of rehabilitation and therapy, a person suffering from a traumatic brain injury may still require daily attendant care and life long medical treatments. The financial costs can be overwhelming for both the victims and their families.
External Injury in Biomechanics
HEAD
Injuries to the head involve the scalp, skull, brain and the nerves and blood vessels entering and exiting the skull. Many studies have documented that these head injuries are frequent, are commonly severe and are as large a cause of death and of disability as are injuries to the rest of the body combined (Gennarelli et al., 1994). The head is the most commonly injured body region and accounts for a large part of resulting impairment and disability.
Biomechanical Issues: A considerable amount of research into the nature and causation of head injuries and a large degree of consensus has been achieved over the basic biomechanical questions. This agreement can be summarised as follows:
• The many different types of head injuries have been described and classified (Graham et al., 2002).
• General agreement has been reached on the severity and the importance of the various types of head injuries regarding the potential for death and disability. These are adequately described in the Abbreviated Injury Scale (Gennarelli et al., 1982, Abbreviated Injury Scale 2005).
• A general understanding exists of the underlying mechanisms that cause altered brain function post injury (Ommaya et al., 2002).
• Frequencies of single and combinations of head injuries have been identified in various injury-producing circumstances.
• The biomechanics of head injuries are reasonably well understood from a qualitative perspective (Goldsmith 2001).
• Regarding the mechanisms and levels of stress or strain that cause injury (i.e., the biomechanical tolerances), there is general agreement regarding scalp injuries and some types of skull injuries.
• There have been estimates from limited sources regarding mechanical tolerances for all head injury globally and for various specific levels of diffuse brain injury (concussions and prolonged traumatic coma) (Gennarelli et al., 2003).
• The applicability of the HIC is limited in understanding certain types of brain injury and there is a need to develop more suitable injury assessment functions.
Head injury criterion
The Head Injury Criterion (HIC) is a measure of the likelihood of head injury arising from an impact. The HIC can be used to assess safety related to vehicles, personal protective gear, and sport equipment.
Normally the variable is derived from the acceleration/time history of an accelerometer mounted at the centre of gravity of a dummy’s head, when the dummy is exposed to crash forces.
It is defined as:
Where t1 and t2 are the initial and final times (in seconds) of the interval during which HIC attains a maximum value, and acceleration a is measured in g's (standard gravity acceleration). Note also the maximum time duration of HIC, t2 - t1, is limited to a specific value, usually 15 ms.
This means that the HIC includes the effects of head acceleration and the duration of the acceleration. Large accelerations may be tolerated for very short times.
At a HIC of 1000, one in six people will suffer a life-threatening injury to their brain (more accurately, an 18% probability of a severe head injury, a 55% probability of a serious injury and a 90% probability of a moderate head injury to the average adult).

NECK INJURIES
Cervical spine distortion (CSD) injuries play a major role in car-to-car collisions worldwide. The high rate of CSD represents not only an economic burden but also a medical challenge. A particular characteristic of so-called “whiplash” injuries is that they can occur in car crashes at low velocity (Krafft et al., 2002). During such an event, vehicle occupants are prone to hyperextension of the neck, particularly at the level of the C6-C7 cervical vertebrae (Kaneoka et al., 1999).
The incidence rate of neck injuries remains high despite the belief that hyperextension of the cervical spine would not occur as long as the occupant is using a head restraint (Lovsund et al., 1988, Olsson et al., 1990, Ono and Kaneoka, 1997). This strongly suggests that factors other than the improper use of head restraints must be involved as a cause of neck injuries. For example, current seat systems including the head restraint are not adequately designed to prevent or mitigate neck injuries.
The potential for long-term impairment, including paraplegia and quadriplegia, is always inherent in injuries to the spine and particularly to the spinal cord. Of all spinal segments, the cervical spine is the region most frequently injured. As the head and the neck form one functional entity, head loading often also implies neck loading and almost always vice versa.
In a rear impact, the occupant is subjected to various forces which tend to differ among individual occupants due to differences in seat position and seat cushion stiffness which are presumably related to the incidence of neck injuries (Lovsund et al., 1988, Olsson et al., 1990, Ono and Kaneoka, 1997, Hell et al., 2003). While research has focused on the relationships between neck muscle responses, motions of cervical vertebrae and injuries to intervertebral discs and articular surfaces, detailed information about these relationships, ranging from relatively minor neck injuries to those resulting in impairment, are still not well understood.
Severe (head-contact) cervical injuries occur to unbelted car occupants not only in rear impacts but also in frontal, lateral and oblique impacts. Half of all minor neck injuries occur in frontal impacts (Hell et al., 2003). The vast majority of cervical spine injuries, however, are minor soft tissue AIS 1 injuries. These injuries, while not associated with overt structural injury to the cervical spine or the central nervous system, are both a common and potentially debilitating injury.
In fact, they are the most frequently occurring injuries in automobile collisions and more often to females than to males (Bunketorp et al., 2004, Jakobsson and Norin, 2004). Thus, soft tissue neck injuries are a major concern in road traffic.
Injury Mechanisms: The mechanisms of the so-called “whiplash” injury have not been clearly understood, and the relationship between the objective physical/medical observations and the subjective symptoms remains unclear (Carlsson et al., 1985, Schrader et al., 1996).
The human neck is a complex structure consisting of skeletal frames, ligaments, blood vessels, muscles and soft tissues such as nerves with diverse strengths. Their forms tend to change continually and in a potentially injury-producing situation, neck muscle strength can depend upon level of consciousness. An impact is transmitted directly to each vertebra or dispersed through the soft tissues, then transmitted to the lower torso. The influence of a head impact on the neck differs significantly depending on the direction of the impact and the orientation of the neck when the impact occurs.
In other words, the neck injury mechanism is roughly classified by the direct transmission of the head impact to the neck (Yamada 1970) and by the inertial head motions around the neck acting as a pivot (Society of Automotive Engineers 1986).
Specific injury mechanisms related to cervical vertebrae are flexion (bending), compression, extension (tension), rotation (torque) or shear force (Figure 1). In general, injuries to the lower vertebral region result from flexion or extension whereas an injury such as a Hangman-type fracture or Jefferson-type fracture, again depending upon the orientation of the neck, results from a shear force. An intervertebral disk or vertebral anterior aspect is likely to be injured by flexion, and the bending moment tends to be greater than in the case of extension. With flexion, however, the impact load against the vertebra changes as the chin contacts the chest (chin-chest impact). In the latter case, the so-called “whiplash” injury may occur without a direct impact to the head. A typical example of such impacts is a vehicle rear-end collision. In the initial stage of a rear-end collision, the occupant’s spinal column is rounded by the seatback reaction force, then straightened upward, causing the torso to move upward along the seatback at the same time. As the head remains in the initial position due to the inertia, an axial compression force is applied to the lower cervical vertebra due to the straightening of the spinal column and the upward motion of the torso. A shear force is then applied to the lower cervical spine due to the collision between the seatback and the upper portion of the torso, resulting in head retroflexional rotation around the lower cervical vertebra acting as the pivot. The phenomena created from the initial impact, the resulting motions of the spinal column and torso, and the retroflexional rotation of the head are becoming more complex due to the specific detail of head restraint installation in recent years.
 Figure 1: Loading patterns for cervical spine
Figure 1: Loading patterns for cervical spine
Generally, the impact time zone during which a neck injury occurs is in the order of several-tens to several-hundred seconds from the moment of impact. The injury severity also depends on the duration of the impact. In some cases, the duration that causes the “whiplash” can be as long as 200ms. These are important considerations to a better understanding of these minor but frequent and sometimes debilitating neck injuries.
Injury Criteria and Tolerance to Injuries: Early work by Yamada (1970) on physical properties and strengths of biological materials such as cervical vertebrae, intervertebral disks and ligaments has contributed significantly to the field of impact biomechanics. Table 1 summarises experimental data on tensile, compression and torsional strengths of vertebrae and the intervetebral discs.
 Table 1: Breaking strength of cervical neck elements in tension, compression and torsion by age group.
Table 1: Breaking strength of cervical neck elements in tension, compression and torsion by age group.
These data are fundamental to the field of impact biomechanics and often referred to as useful data in various other fields. The injuries that occur in line with the flexion, compression, torsion and/or shear forces applied to the cervical vertebrae described above are classified (Society of Automotive Engineers 1986) and shown in Table 2.
 Table 2: Types of neck injuries based on neck injury mechanisms
Table 2: Types of neck injuries based on neck injury mechanisms
Mertz and Chou (1976) proposed neck injury tolerance curves in 1976 based on experimental data from volunteers and cadavers. These curves determine the limits for torque, flexion angle and extension angles relative to the occipital condyle.
The test data of axial load, shear force and bending torque are summarized and shown in Table 3.
 Table 3: Maximum static forces and bending torques developed at the occipital condyles by human volunteers.
Table 3: Maximum static forces and bending torques developed at the occipital condyles by human volunteers.
Moreover, Mertz (1990) also proposed neck injury criteria based on dynamic experiments conducted using cadavers, and accident simulations using Hybrid III dummies. The proposed tolerance level to the occipital condyle torque is 190 Nm for the forward flexion, and 57 Nm for the backward extension. These injury criteria are applied at present to the evaluation of neck injuries in automobile safety evaluation tests using the Hybrid-III crash test dummy. Injury criteria values for axial compression, tension and shear force are shown in Figure 2.
 Figure 2: Neck Injury Criteria for ATD dummy
Figure 2: Neck Injury Criteria for ATD dummy
It should be noted, however, that the data obtained with these injury criteria values are applicable mainly to experiments and studies on head inertia loads. These values do not provide injury criteria for human biological impact responses where human heads are subjected to direct impacts (Xu et al., 2000). The values being used at present as the injury criteria (Federal Register 2000) are listed in Table 4.
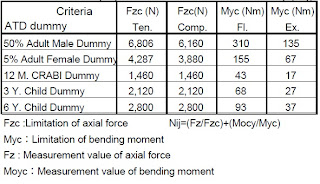 Table 4: Neck injury criteria based on ATD dummy (Nij)
Table 4: Neck injury criteria based on ATD dummy (Nij)
Recently, quite extensive studies on minor neck injury (i.e., “whiplash”) caused by head inertial impacts were conducted in addition to the above, and the “whiplash” injury evaluation parameters and the criteria are proposed as shown in Table 5 (IIWPG 2001).
 Table 5: Proposed Injury Evaluation Parameters and Injury Criterion for Whiplash Prevention
Table 5: Proposed Injury Evaluation Parameters and Injury Criterion for Whiplash Prevention
Injuries to the head involve the scalp, skull, brain and the nerves and blood vessels entering and exiting the skull. Many studies have documented that these head injuries are frequent, are commonly severe and are as large a cause of death and of disability as are injuries to the rest of the body combined (Gennarelli et al., 1994). The head is the most commonly injured body region and accounts for a large part of resulting impairment and disability.
Biomechanical Issues: A considerable amount of research into the nature and causation of head injuries and a large degree of consensus has been achieved over the basic biomechanical questions. This agreement can be summarised as follows:
• The many different types of head injuries have been described and classified (Graham et al., 2002).
• General agreement has been reached on the severity and the importance of the various types of head injuries regarding the potential for death and disability. These are adequately described in the Abbreviated Injury Scale (Gennarelli et al., 1982, Abbreviated Injury Scale 2005).
• A general understanding exists of the underlying mechanisms that cause altered brain function post injury (Ommaya et al., 2002).
• Frequencies of single and combinations of head injuries have been identified in various injury-producing circumstances.
• The biomechanics of head injuries are reasonably well understood from a qualitative perspective (Goldsmith 2001).
• Regarding the mechanisms and levels of stress or strain that cause injury (i.e., the biomechanical tolerances), there is general agreement regarding scalp injuries and some types of skull injuries.
• There have been estimates from limited sources regarding mechanical tolerances for all head injury globally and for various specific levels of diffuse brain injury (concussions and prolonged traumatic coma) (Gennarelli et al., 2003).
• The applicability of the HIC is limited in understanding certain types of brain injury and there is a need to develop more suitable injury assessment functions.
Head injury criterion
The Head Injury Criterion (HIC) is a measure of the likelihood of head injury arising from an impact. The HIC can be used to assess safety related to vehicles, personal protective gear, and sport equipment.
Normally the variable is derived from the acceleration/time history of an accelerometer mounted at the centre of gravity of a dummy’s head, when the dummy is exposed to crash forces.
It is defined as:
Where t1 and t2 are the initial and final times (in seconds) of the interval during which HIC attains a maximum value, and acceleration a is measured in g's (standard gravity acceleration). Note also the maximum time duration of HIC, t2 - t1, is limited to a specific value, usually 15 ms.
This means that the HIC includes the effects of head acceleration and the duration of the acceleration. Large accelerations may be tolerated for very short times.
At a HIC of 1000, one in six people will suffer a life-threatening injury to their brain (more accurately, an 18% probability of a severe head injury, a 55% probability of a serious injury and a 90% probability of a moderate head injury to the average adult).

NECK INJURIES
Cervical spine distortion (CSD) injuries play a major role in car-to-car collisions worldwide. The high rate of CSD represents not only an economic burden but also a medical challenge. A particular characteristic of so-called “whiplash” injuries is that they can occur in car crashes at low velocity (Krafft et al., 2002). During such an event, vehicle occupants are prone to hyperextension of the neck, particularly at the level of the C6-C7 cervical vertebrae (Kaneoka et al., 1999).
The incidence rate of neck injuries remains high despite the belief that hyperextension of the cervical spine would not occur as long as the occupant is using a head restraint (Lovsund et al., 1988, Olsson et al., 1990, Ono and Kaneoka, 1997). This strongly suggests that factors other than the improper use of head restraints must be involved as a cause of neck injuries. For example, current seat systems including the head restraint are not adequately designed to prevent or mitigate neck injuries.
The potential for long-term impairment, including paraplegia and quadriplegia, is always inherent in injuries to the spine and particularly to the spinal cord. Of all spinal segments, the cervical spine is the region most frequently injured. As the head and the neck form one functional entity, head loading often also implies neck loading and almost always vice versa.
In a rear impact, the occupant is subjected to various forces which tend to differ among individual occupants due to differences in seat position and seat cushion stiffness which are presumably related to the incidence of neck injuries (Lovsund et al., 1988, Olsson et al., 1990, Ono and Kaneoka, 1997, Hell et al., 2003). While research has focused on the relationships between neck muscle responses, motions of cervical vertebrae and injuries to intervertebral discs and articular surfaces, detailed information about these relationships, ranging from relatively minor neck injuries to those resulting in impairment, are still not well understood.
Severe (head-contact) cervical injuries occur to unbelted car occupants not only in rear impacts but also in frontal, lateral and oblique impacts. Half of all minor neck injuries occur in frontal impacts (Hell et al., 2003). The vast majority of cervical spine injuries, however, are minor soft tissue AIS 1 injuries. These injuries, while not associated with overt structural injury to the cervical spine or the central nervous system, are both a common and potentially debilitating injury.
In fact, they are the most frequently occurring injuries in automobile collisions and more often to females than to males (Bunketorp et al., 2004, Jakobsson and Norin, 2004). Thus, soft tissue neck injuries are a major concern in road traffic.
Injury Mechanisms: The mechanisms of the so-called “whiplash” injury have not been clearly understood, and the relationship between the objective physical/medical observations and the subjective symptoms remains unclear (Carlsson et al., 1985, Schrader et al., 1996).
The human neck is a complex structure consisting of skeletal frames, ligaments, blood vessels, muscles and soft tissues such as nerves with diverse strengths. Their forms tend to change continually and in a potentially injury-producing situation, neck muscle strength can depend upon level of consciousness. An impact is transmitted directly to each vertebra or dispersed through the soft tissues, then transmitted to the lower torso. The influence of a head impact on the neck differs significantly depending on the direction of the impact and the orientation of the neck when the impact occurs.
In other words, the neck injury mechanism is roughly classified by the direct transmission of the head impact to the neck (Yamada 1970) and by the inertial head motions around the neck acting as a pivot (Society of Automotive Engineers 1986).
Specific injury mechanisms related to cervical vertebrae are flexion (bending), compression, extension (tension), rotation (torque) or shear force (Figure 1). In general, injuries to the lower vertebral region result from flexion or extension whereas an injury such as a Hangman-type fracture or Jefferson-type fracture, again depending upon the orientation of the neck, results from a shear force. An intervertebral disk or vertebral anterior aspect is likely to be injured by flexion, and the bending moment tends to be greater than in the case of extension. With flexion, however, the impact load against the vertebra changes as the chin contacts the chest (chin-chest impact). In the latter case, the so-called “whiplash” injury may occur without a direct impact to the head. A typical example of such impacts is a vehicle rear-end collision. In the initial stage of a rear-end collision, the occupant’s spinal column is rounded by the seatback reaction force, then straightened upward, causing the torso to move upward along the seatback at the same time. As the head remains in the initial position due to the inertia, an axial compression force is applied to the lower cervical vertebra due to the straightening of the spinal column and the upward motion of the torso. A shear force is then applied to the lower cervical spine due to the collision between the seatback and the upper portion of the torso, resulting in head retroflexional rotation around the lower cervical vertebra acting as the pivot. The phenomena created from the initial impact, the resulting motions of the spinal column and torso, and the retroflexional rotation of the head are becoming more complex due to the specific detail of head restraint installation in recent years.

Generally, the impact time zone during which a neck injury occurs is in the order of several-tens to several-hundred seconds from the moment of impact. The injury severity also depends on the duration of the impact. In some cases, the duration that causes the “whiplash” can be as long as 200ms. These are important considerations to a better understanding of these minor but frequent and sometimes debilitating neck injuries.
Injury Criteria and Tolerance to Injuries: Early work by Yamada (1970) on physical properties and strengths of biological materials such as cervical vertebrae, intervertebral disks and ligaments has contributed significantly to the field of impact biomechanics. Table 1 summarises experimental data on tensile, compression and torsional strengths of vertebrae and the intervetebral discs.

These data are fundamental to the field of impact biomechanics and often referred to as useful data in various other fields. The injuries that occur in line with the flexion, compression, torsion and/or shear forces applied to the cervical vertebrae described above are classified (Society of Automotive Engineers 1986) and shown in Table 2.

Mertz and Chou (1976) proposed neck injury tolerance curves in 1976 based on experimental data from volunteers and cadavers. These curves determine the limits for torque, flexion angle and extension angles relative to the occipital condyle.
The test data of axial load, shear force and bending torque are summarized and shown in Table 3.

Moreover, Mertz (1990) also proposed neck injury criteria based on dynamic experiments conducted using cadavers, and accident simulations using Hybrid III dummies. The proposed tolerance level to the occipital condyle torque is 190 Nm for the forward flexion, and 57 Nm for the backward extension. These injury criteria are applied at present to the evaluation of neck injuries in automobile safety evaluation tests using the Hybrid-III crash test dummy. Injury criteria values for axial compression, tension and shear force are shown in Figure 2.

It should be noted, however, that the data obtained with these injury criteria values are applicable mainly to experiments and studies on head inertia loads. These values do not provide injury criteria for human biological impact responses where human heads are subjected to direct impacts (Xu et al., 2000). The values being used at present as the injury criteria (Federal Register 2000) are listed in Table 4.

Recently, quite extensive studies on minor neck injury (i.e., “whiplash”) caused by head inertial impacts were conducted in addition to the above, and the “whiplash” injury evaluation parameters and the criteria are proposed as shown in Table 5 (IIWPG 2001).

Monday 20 June 2011
Injury Biomechanics
Frequently biomechanical engineers are the best experts to address and explain the entire range of trauma of an injured person, because they are not focused solely on the injury. Rather, they look at the internal and external forces that created the trauma. This includes the event itself, as well as objects involved, such as vehicles, tools, machines or weapons. They also consider the post event stresses of rehabilitation, and the implications of patient non-compliance. Human biomechanical data is generated by measuring and mathematical modeling activities. Biomechanical engineering is a vital aspect of many types of cases, including, but not limited to, vehicle collisions, slip and falls, sports and recreational injuries, medical devices, consumer and commercial products, industrial and construction injuries, as well as burns and scalding.
Injury patterns tell a story about the injury event motion (or kinetics) as well as the magnitude and direction of the force. Traditional mechanical analyses are used to determine external forces applied to the body or vehicle and biomechanical analyses are used to determine the internal forces and reactions of the human body to the external and internal forces.
Injury patterns tell a story about the injury event motion (or kinetics) as well as the magnitude and direction of the force. Traditional mechanical analyses are used to determine external forces applied to the body or vehicle and biomechanical analyses are used to determine the internal forces and reactions of the human body to the external and internal forces.
Monday 13 June 2011
Introduction for Biomechanics Part II
People become injured every day. When you become involved, are you asking the question?
“Are the injuries consistent with the description of the incident?”
Oftentimes, lawsuits focus on product defects, premises liability, supervision issues, code or standards violations and many more without a thorough examination of the fundamental physical processes that are responsible for the injury, and whether the injury is consistent with first-hand accounts.
Biomechanics is the science that studies the external action of energy and forces acting on living bodies, especially the skeletal system. A Forensic Biomechanist is proficient at conducting biomechanical injury analysis investigations, describing the mechanism of injury, providing technical analysis and presenting it during litigation proceedings.
Simply put, biomechanics is a science that combines the principles of mechanical engineering and the study of the human body allowing the biomechanical expert to understand how muscles, tissues, tendons and bones will react to a given force. Consequently, this science gives forensics a tool to answer the question, "Is there a mechanism for injury in the claimed incident?"

“Are the injuries consistent with the description of the incident?”
Oftentimes, lawsuits focus on product defects, premises liability, supervision issues, code or standards violations and many more without a thorough examination of the fundamental physical processes that are responsible for the injury, and whether the injury is consistent with first-hand accounts.
Biomechanics is the science that studies the external action of energy and forces acting on living bodies, especially the skeletal system. A Forensic Biomechanist is proficient at conducting biomechanical injury analysis investigations, describing the mechanism of injury, providing technical analysis and presenting it during litigation proceedings.
Simply put, biomechanics is a science that combines the principles of mechanical engineering and the study of the human body allowing the biomechanical expert to understand how muscles, tissues, tendons and bones will react to a given force. Consequently, this science gives forensics a tool to answer the question, "Is there a mechanism for injury in the claimed incident?"

Introduction for Biomechanics Part I
Biomechanics is the application of mechanical principles to biological systems, such as humans, animals, plants, organs, and cells. Perhaps one of the best definitions was provided by Herbert Hatze in 1974: "Biomechanics is the study of the structure and function of biological systems by means of the methods of mechanics". The word biomechanics developed during the early 1970s, describing the application of engineering mechanics to biological and medical systems.

Biomechanics is closely related to engineering, because it often uses traditional engineering sciences to analyse biological systems. Some simple applications of Newtonian mechanics and/or materials sciences can supply correct approximations to the mechanics of many biological systems. Applied mechanics, most notably mechanical engineering disciplines such as continuum mechanics, mechanism analysis, structural analysis, kinematics and dynamics play prominent roles in the study of biomechanics.
Usually biological systems are more complex than man-built systems. Numerical methods are hence applied in almost every biomechanical study. Research is done in a iterative process of hypothesis and verification, including several steps of modelling, computer simulation and experimental measurements.
A field that combines the disciplines of biology and engineering mechanics and utilizes the tools of physics, mathematics, and engineering to quantitatively describe the properties of biological materials. One of its basic properties is embodied in so-called constitutive laws, which fundamentally describe the properties of constituents, independent of size or geometry, and specifically how a material deforms in response to applied forces. For most inert materials, measurement of the forces and deformations is straightforward by means of commercially available devices or sensors that can be attached to a test specimen. Many materials, ranging from steel to rubber, have linear constitutive laws, with the proportionality constant (elastic modulus) between the deformation and applied forces providing a simple index to distinguish the soft rubber from the stiff steel. While the same basic principles apply to living tissues, the complex composition of tissues makes obtaining constitutive laws difficult.

The biomechanical properties and behaviors of organs and organ systems stem from the ensemble characteristics of their component cells and extracellular materials, which vary widely in structure and composition and hence in biomechanical properties. An example of this complexity is provided by the cardiovascular system, which is composed of the heart, blood vessels, and blood.

Biomechanics is closely related to engineering, because it often uses traditional engineering sciences to analyse biological systems. Some simple applications of Newtonian mechanics and/or materials sciences can supply correct approximations to the mechanics of many biological systems. Applied mechanics, most notably mechanical engineering disciplines such as continuum mechanics, mechanism analysis, structural analysis, kinematics and dynamics play prominent roles in the study of biomechanics.
Usually biological systems are more complex than man-built systems. Numerical methods are hence applied in almost every biomechanical study. Research is done in a iterative process of hypothesis and verification, including several steps of modelling, computer simulation and experimental measurements.
A field that combines the disciplines of biology and engineering mechanics and utilizes the tools of physics, mathematics, and engineering to quantitatively describe the properties of biological materials. One of its basic properties is embodied in so-called constitutive laws, which fundamentally describe the properties of constituents, independent of size or geometry, and specifically how a material deforms in response to applied forces. For most inert materials, measurement of the forces and deformations is straightforward by means of commercially available devices or sensors that can be attached to a test specimen. Many materials, ranging from steel to rubber, have linear constitutive laws, with the proportionality constant (elastic modulus) between the deformation and applied forces providing a simple index to distinguish the soft rubber from the stiff steel. While the same basic principles apply to living tissues, the complex composition of tissues makes obtaining constitutive laws difficult.

The biomechanical properties and behaviors of organs and organ systems stem from the ensemble characteristics of their component cells and extracellular materials, which vary widely in structure and composition and hence in biomechanical properties. An example of this complexity is provided by the cardiovascular system, which is composed of the heart, blood vessels, and blood.
Blog Assignment - Objective
This blog assignment is where the students blend the course material into their world. Unlike the research paper, blog posts are low-stakes writing, hence it's okay if the organization is more exploratory than structured.
From this task, we're taking topic that called Biomechanics. In this group we've 7 persons and each of them have been given a task about Biomechanics.
Objective :
- Students able to discuss, reflect and demonstrate connections and ongoing engagement with the materials of this course such as readings, websites and lectures
- Students will be using a class blog in this course as a medium for critique and reflection and for sharing ideas and information relevant to the course and particularly topics chosen

From this task, we're taking topic that called Biomechanics. In this group we've 7 persons and each of them have been given a task about Biomechanics.
Objective :
- Students able to discuss, reflect and demonstrate connections and ongoing engagement with the materials of this course such as readings, websites and lectures
- Students will be using a class blog in this course as a medium for critique and reflection and for sharing ideas and information relevant to the course and particularly topics chosen

Subscribe to:
Posts (Atom)